Climbing is quickly becoming one of the most popular sports in the world. Who isn’t intrigued by the exciting free solo ascent by Alex Honnald or Margo Hayes ticking yet another 5.15a (super super hard climb) at the age of 21?
As exciting as climbing is, it’s extremely challenging and requires both mental and physical strength. Weekly training, bouldering and hangboard sessions can advance your grade, but if done without care may lead to injury. Many climbers have experienced the dreaded twinge on the inside of their elbow during or after training. If left unchecked this pain can become increasingly sore, weaken the grip, and make climbing near impossible. This 3-part series will look at why medial elbow pain occurs in climbers and what we can do about it.
Part 1 – Medial Elbow Pain
Medial epicondyle tendinopathy is typically an overload injury that leads to pain in the elbow. Sometimes called golfers elbow (climbers elbow) it is prominent in climber’s due to the demands of the sport and our bodies ability to adapt.
When we climb our palms are usually turned away from our bodies with finger and wrist in a flexed position. The muscles that flex the wrist and fingers (such as the flexor digitorum) and the muscle that turns our palms away (pronator teres) attach on the inside of the elbow on an area called the medial epicondyle.
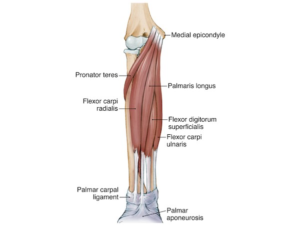
source: https://pathologies.lexmedicus.com.au
In climbing, we flex our wrist and fingers over the rock and pull down to leverage our body weight upward. This transmits force through that small area of muscle attachment. Over time the repetitive loading can go beyond the capacity of the tendon. Risk factors for this injury are over training, new climbers, poor technique, fatigue and fear (such as clipping after a run out) that leads to over gripping the rock creating more load than needed.
Another reason why medial epicondyle tendinopathy is prominent in climbers is the adaptation of the body. As we train our muscles get stronger and grow to meet the capacity of their demand. This is why you see more experienced climbers with well-defined forearms. However, tendons growth and strength takes more time to develop then muscles. Research shows a significant lag in time for tendon strength to develop behind muscles.

So, as the muscles get stronger and can pull more, the tendon can’t keep up with the demand leading increased force in the elbow and ultimately, that inside elbow pain. This is why patience, progressive tendon loading and developing good technique is essential in training.
One of the early signs of medial epicondyle tendinopathy include an ache inside the elbow at the beginning of a training session that settles down after warming up. Climbers might experience pain to touch at the inside elbow, stiffness with movement or weakness in the hand or wrist. Pain can often be reproduced with resisted flexion and rotation of the wrist during testing with your Physio.
Often the pain may come on, settle and go away, but more commonly climbers will have reoccurring discomfort that increases in pain and takes longer to settle. As the tendon continues to be loaded beyond its capacity the collagen fibres in the tendon can become thickened with an increase in mucoid ground substance. The cells of the tendon take on a watery texture and the collagen loses some its strength. If managed well, this process can be relatively short term and the tendon can increase in stiffness and be able to adapt to greater load. However, without proper rehab and Physio treatment, the collagen wear increases and the cells in the tendon loses their shape leading to further pain and reduced tendon capacity.
If you have elbow pain on the inside of your elbow come and see one of our Physio’s here at Bend + Mend for expert management so you can climb again soon!
Part two looks at some key steps of treatment to get you back on the wall.
References:
Brumitt, J., & Cuddeford, T. (2015). Current concepts of muscle and tendon adaptation to strength and conditioning. International journal of sports physical therapy, 10(6), 748
Mersmann, F., Bohm, S., & Arampatzis, A. (2017). Imbalances in the development of muscle and tendon as risk factor for tendinopathies in youth athletes: a review of current evidence and concepts of prevention. Frontiers in physiology, 8, 987.
Rooks, M. D. (1997). Rock climbing injuries. Sports medicine, 23(4), 261-270.